Recent Medicaid policy changes enacted through Idaho Public Law 119-21 and House Bill 345 represent a substantive shift in the structure of healthcare access for low-income populations. While these policies are framed as mechanisms to promote workforce participation and reduce public expenditures, they simultaneously introduce administrative conditions that may function as barriers to care. From a public health perspective, the implications of these changes extend beyond eligibility criteria and into broader domains of health equity, access, and population-level outcomes.
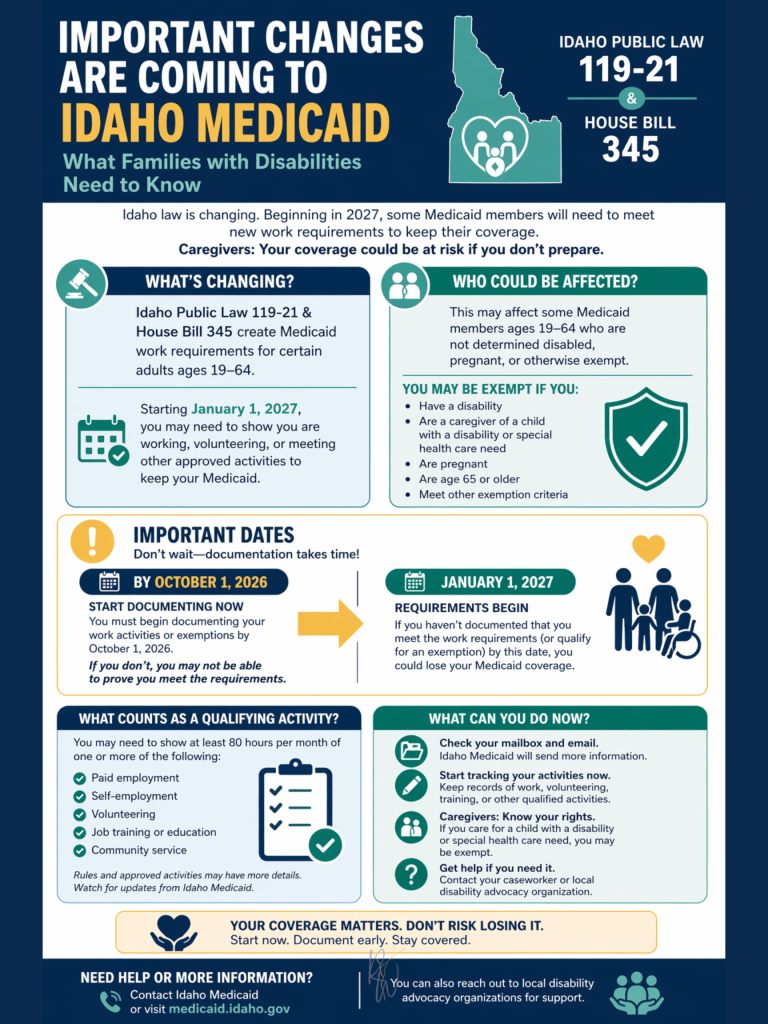
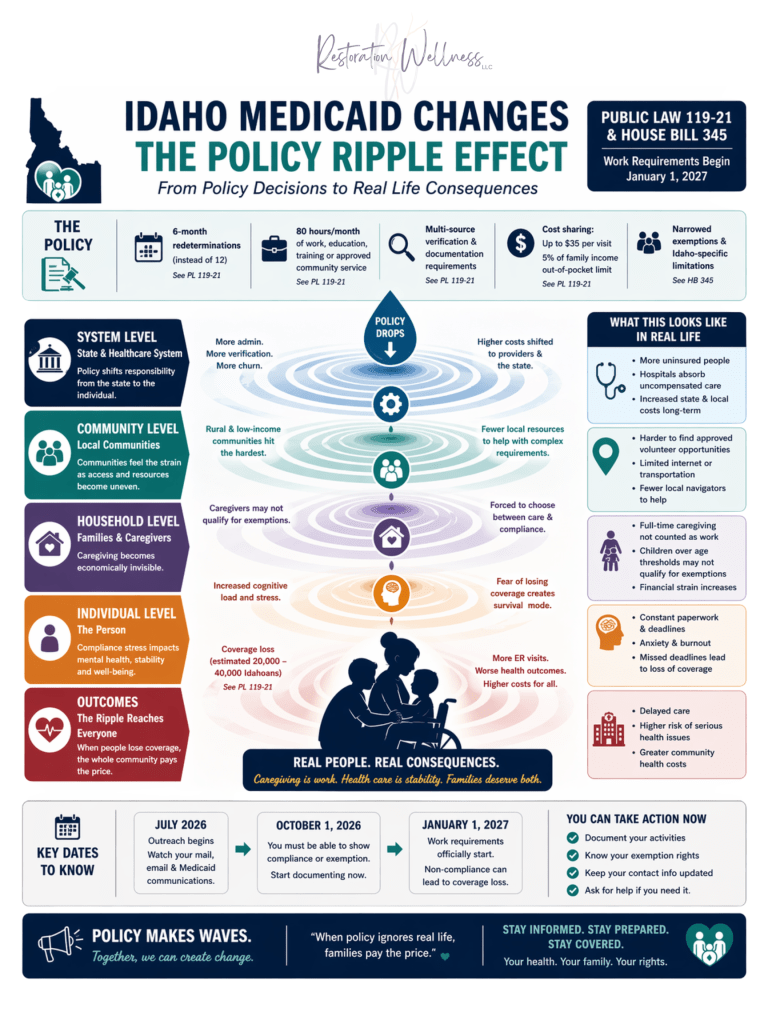
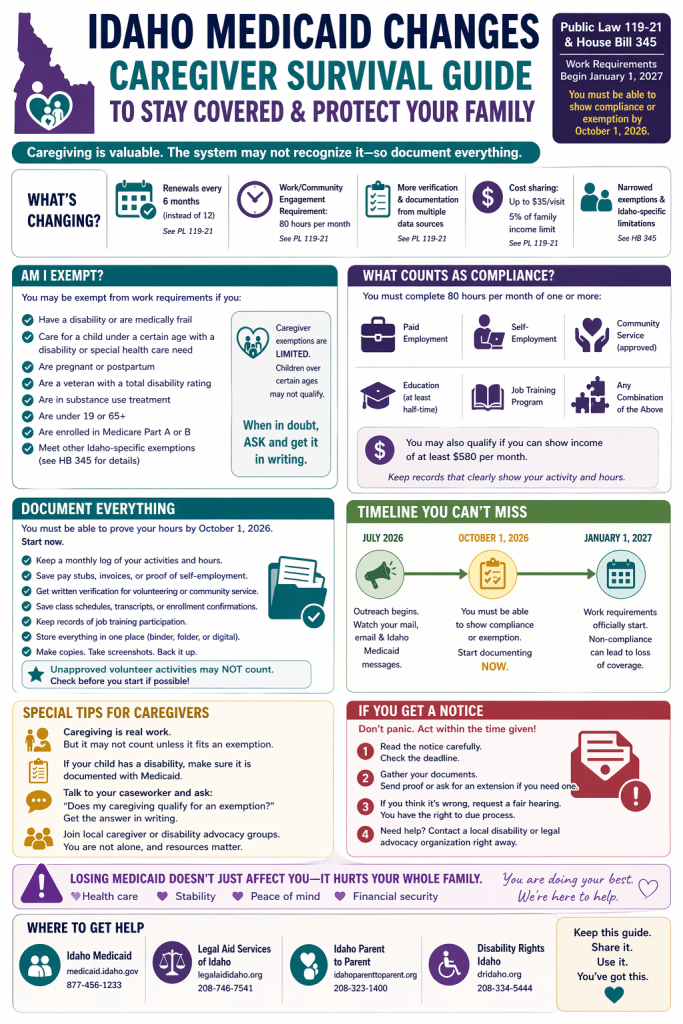
Historically, Medicaid eligibility in Idaho has been governed by statutory authority under Idaho Code §56-267, which established coverage for low-income adults under expansion provisions. Eligibility determinations have traditionally relied on income thresholds and categorical qualifications, with annual redetermination processes designed to maintain continuity of care. However, recent policy changes introduce a conditional compliance framework in which eligibility must be continuously demonstrated through documented participation in qualifying activities. These include employment, education, job training, or approved community engagement, generally defined as approximately eighty hours per month. Additionally, eligibility redetermination is now required every six months rather than annually, increasing the frequency of administrative review (Idaho Code §56-209; Idaho Code §56-201; Kidney, 2026).
This shift reflects a broader national trend toward incorporating “community engagement” requirements into Medicaid through Section 1115 demonstration waivers (Centers for Medicare & Medicaid Services [CMS], n.d.). While such policies are often justified as promoting self-sufficiency, empirical evidence suggests that their primary effect may be increased administrative complexity rather than sustained employment gains. In Arkansas, the first state to implement Medicaid work requirements, coverage losses were significant, while measurable improvements in employment were not observed (Sommers et al., 2019).
Administrative burden provides a critical framework for understanding these outcomes. Defined as the learning, compliance, and psychological costs associated with navigating public programs, administrative burden operates as a hidden but powerful determinant of access (Herd & Moynihan, 2018). These burdens are not distributed equally. Individuals with stable housing, consistent internet access, flexible employment, and higher levels of administrative literacy are more likely to maintain compliance. Conversely, individuals experiencing socioeconomic disadvantage, disability, or caregiving demands face increased risk of coverage loss due to procedural barriers rather than ineligibility (Herd & Moynihan, 2018; Sommers et al., 2019).
This dynamic is not theoretical. As a caregiver to multiple children with disabilities, I operate within this system in real time. Maintaining eligibility is not a singular administrative task but an ongoing process requiring continuous documentation, monitoring, and responsiveness across multiple systems. These requirements exist alongside full-time caregiving responsibilities, where time, attention, and cognitive bandwidth are already fully allocated. The expectation that individuals in similar positions can consistently meet these administrative thresholds without disruption does not reflect the functional realities of caregiving.
In Idaho’s current framework, compliance requires individuals to track qualifying activities, interpret eligibility criteria, submit documentation through state-approved systems, and respond to outreach within defined timelines. The requirement to demonstrate compliance by October 1, 2026, prior to enforcement in January 2027, reinforces the expectation of continuous administrative engagement (Kidney, 2026). From a public health standpoint, this transforms Medicaid eligibility into an ongoing procedural obligation rather than a stable access point.
The implications of this shift are particularly significant for families caring for individuals with disabilities. While Idaho policy includes exemptions for certain populations, including those who are medically frail or serving as caregivers, House Bill 345 introduces state-specific limitations that may narrow the scope of these exemptions. Variations in how disability is defined and verified, as well as restrictions tied to caregiver status, create a disconnect between functional caregiving responsibilities and formal recognition within the system (Kidney, 2026).
In my own experience as a parent of children with complex needs, caregiving is neither passive nor incidental. It is structured, intensive, and often medically adjacent labor. However, within current policy frameworks, this labor is not consistently recognized unless it aligns with narrowly defined exemption criteria. This creates a structural misalignment in which full-time caregiving may coexist with additional work requirements, effectively requiring individuals to produce both unpaid and externally validated labor to maintain access to healthcare.
From a public health perspective, this represents a critical misclassification of labor. Caregiving contributes directly to health maintenance, reduces institutional care costs, and supports broader system stability. When such labor is excluded from qualifying activity, policy frameworks fail to account for one of the most essential forms of health-supporting work within communities.
Evidence from prior Medicaid work requirement implementations further underscores these concerns. In Arkansas, individuals who lost coverage were often already working or qualified for exemptions but failed to successfully navigate reporting requirements (Sommers et al., 2019). These findings indicate that administrative complexity, rather than lack of engagement, is a primary driver of coverage loss.
The cognitive and psychological dimensions of administrative burden further compound these effects. Compliance systems require sustained executive functioning, including organization, planning, and timely response to administrative demands. Chronic stress, which disproportionately affects low-income populations and caregivers, is associated with reduced cognitive capacity and impaired decision-making (Mullainathan & Shafir, 2013). As a result, individuals facing the greatest structural challenges are often the least equipped to meet compliance requirements, creating a feedback loop in which vulnerability increases the likelihood of coverage loss.
At the population level, the consequences of reduced Medicaid coverage extend beyond individual outcomes. Loss of coverage is associated with decreased access to preventive services, increased reliance on emergency care, and higher levels of uncompensated care within healthcare systems (Sommers et al., 2017). Idaho estimates that between 20,000 and 40,000 individuals may lose coverage under the current policy framework (Kidney, 2026). These losses do not reflect reduced healthcare need but rather a shift in how and where care is accessed, often at greater cost and reduced efficiency.
The introduction of cost-sharing provisions further complicates access. Although capped at five percent of household income, even modest out-of-pocket costs can deter healthcare utilization among low-income populations (Sommers et al., 2017). When combined with administrative requirements, these financial barriers contribute to a cumulative effect in which access to care becomes increasingly conditional.
From both a professional and personal standpoint, this issue extends beyond policy analysis. It reflects a growing tension between systems designed to provide support and the lived realities of those expected to navigate them. When individuals who are already operating at capacity are required to continuously prove eligibility for care, the system risks shifting from a source of stability to a source of strain.
Ultimately, these policy changes reflect a broader transformation in the role of Medicaid. Rather than functioning solely as a safety net based on need, the program is increasingly structured around continuous demonstration of compliance. While accountability and engagement are legitimate policy objectives, they must be balanced against the foundational purpose of Medicaid: to provide access to care for vulnerable populations.
When access depends more on administrative navigation than on medical or socioeconomic need, the system does not simply become more structured. It becomes a gatekeeping function designed to protect a balanced budget. It becomes selective.
Call to Action: Engaging with Idaho’s Legislative Process
Policy is not static. It is responsive to constituent input, particularly at the state level. Idaho residents have the ability to directly engage with their elected officials regarding the implementation and impact of Medicaid policy changes.
To identify and contact your legislative representatives, you can use the official Idaho Legislature website:
This tool allows you to locate your district representatives and senators by entering your home address.
When contacting legislators, consider addressing the following:
- The impact of administrative burden on Medicaid access
- The need for broader recognition of caregiving as qualifying labor
- Snailmail vs email (thrown in an automated junk bin) makes a lasting impact!
- Concerns regarding six-month redetermination cycles
- The potential for coverage loss due to documentation barriers rather than ineligibility
- The public health consequences of reduced access to care
Communication can be made through email, phone, or formal written correspondence. Clear, concise, and experience-informed input is often the most effective.
“This analysis integrates Idaho statutory law, state implementation materials, and professional seminar interpretation to evaluate public health impact.”
Sources
Idaho Legislature. (2025). Public Law 119-21: Working Family Tax Cut Legislation. State of Idaho. Available at: https://legislature.idaho.gov
Idaho Legislature. (2025). House Bill 345. State of Idaho. Available at: https://legislature.idaho.gov
Idaho Code §56-267. Optional Medicaid Expansion.
Idaho Code §56-209. Powers and Duties of the Department of Health and Welfare.
Idaho Code §56-201. Eligibility Determinations and Required Information.
Idaho Code §56-105. Administration of Public Assistance Programs.
Idaho Department of Health and Welfare. (2026). Medicaid Program Guidance and Eligibility Requirements. Available at: https://healthandwelfare.idaho.gov
Centers for Medicare & Medicaid Services. (n.d.). Section 1115 Demonstration Waivers. U.S. Department of Health and Human Services. Available at: https://www.medicaid.gov
Kidney, C. (2026). The Impact of Medicaid Legislation and Policy on Public Health in Idaho [Seminar].
Discover more from
Subscribe to get the latest posts sent to your email.
